
Lessons learnt from 28 Stroke Survivors Testing Our XR + FES Rehabilitation System.
May 27, 2026
This blog post describes how v-health XR enables ADAPTIVE therapy for patients with different mobility levels.
Stroke rehabilitation is hard. Not just physically hard — repetitive, exhausting, frustrating hard. Hard commercially and clinically.
Despite decades of progress in neuroscience and rehabilitation, many stroke survivors still receive far less upper limb therapy than the government recommends. Recovery often becomes limited not by potential, but by time, intensity, motivation, staffing, and access.
That’s where v-health XR comes in.
What is v-health XR?
v-health XR is our immersive neurorehabilitation platform combining:
Extended Reality (XR)
Functional Electrical Stimulation (FES)
Real-time hand tracking
Gamified rehabilitation experiences
In simple terms:
Patients wear lightweight muscle stimulation devices (eir bands) and an XR headset (Meta Quest or others). As they move, or attempt to move, the system reacts in real time with synchronized stimulation and interactive virtual experiences.
Think:
catching virtual fish,
controlling a flying phoenix,
or stacking pieces of a 3D puzzle in mixed reality to create a swan, while your muscles receive adaptive assistance.
You can read more about the games in one of our previous blog posts: here & here.

Figure 1. A stroke survivor experiences v-health XR at one of the study site. They wear an XR headset and FES wearables, eir bands.
The Study
We recently completed a multi-site feasibility study with:
28 chronic stroke survivors
4 clinical sites across the UK
participants ranging from mild to severe upper limb impairment
Sessions lasted up to ~30 minutes, with participants trying multiple XR rehabilitation games targeting:
wrist extension,
wrist flexion,
hand opening,
grasping,
and arm movement.
The study was approved by the NHS HRA ethics committee. A scientific publication for this study is currently in preparation.
v-health XR showed high usability
First of all, the usability of the v-health XR was high (measured by VR system usability questionnaire) - around 75%. (Figure 2). Second, usability didn’t depend on the participants’ motor ability (FMA score)! In many other modern intervention studies, participants with low mobility find it difficult to engage with technology. Our case showed that both low mobility users (FMA < 20) as well as high mobility users (FMA > 50) had high engagement with the system.

Figure 1. VR system usabilily as a function of FMA score. The trend line doesn’t show any dependence of the usability on the FMA.
Different Patients Preferred Different Games.
This turned out to be much more important than we initially expected.
Participants with more severe motor impairment (lower FMA, or Fugl-Meyer Assessment, score) tended to prefer simpler, more assistive experiences like Rise of the Phoenix (Figure 3a), where wrist extension controlled the flight of a bird through floating rings.
Participants with higher motor ability (higher FMA, or Fugl-Meyer Assessment, score) often preferred more complex interaction-heavy tasks like Place the Cubes (Figure 3c), which involved grasping, releasing, and coordinated arm movement.
In other words:
Different impairment levels naturally gravitated toward different XR interaction styles.
This may sound obvious in hindsight, but it has major implications for adaptive rehabilitation design.

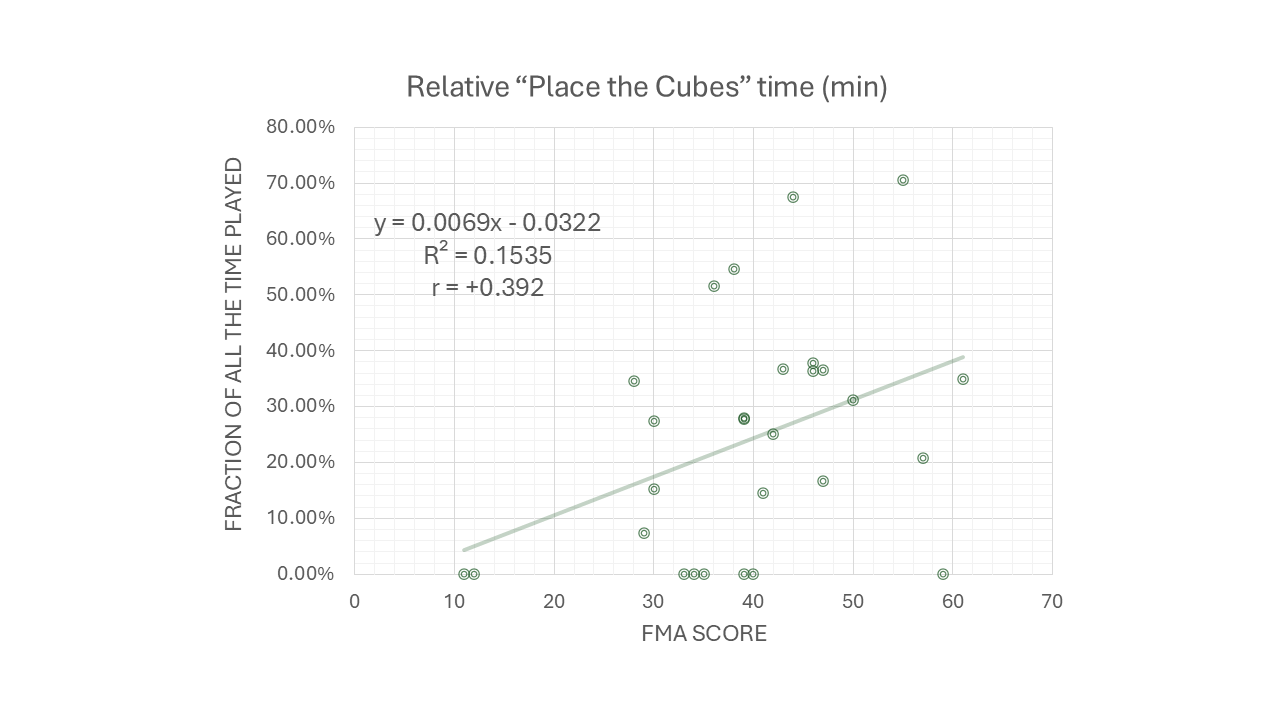
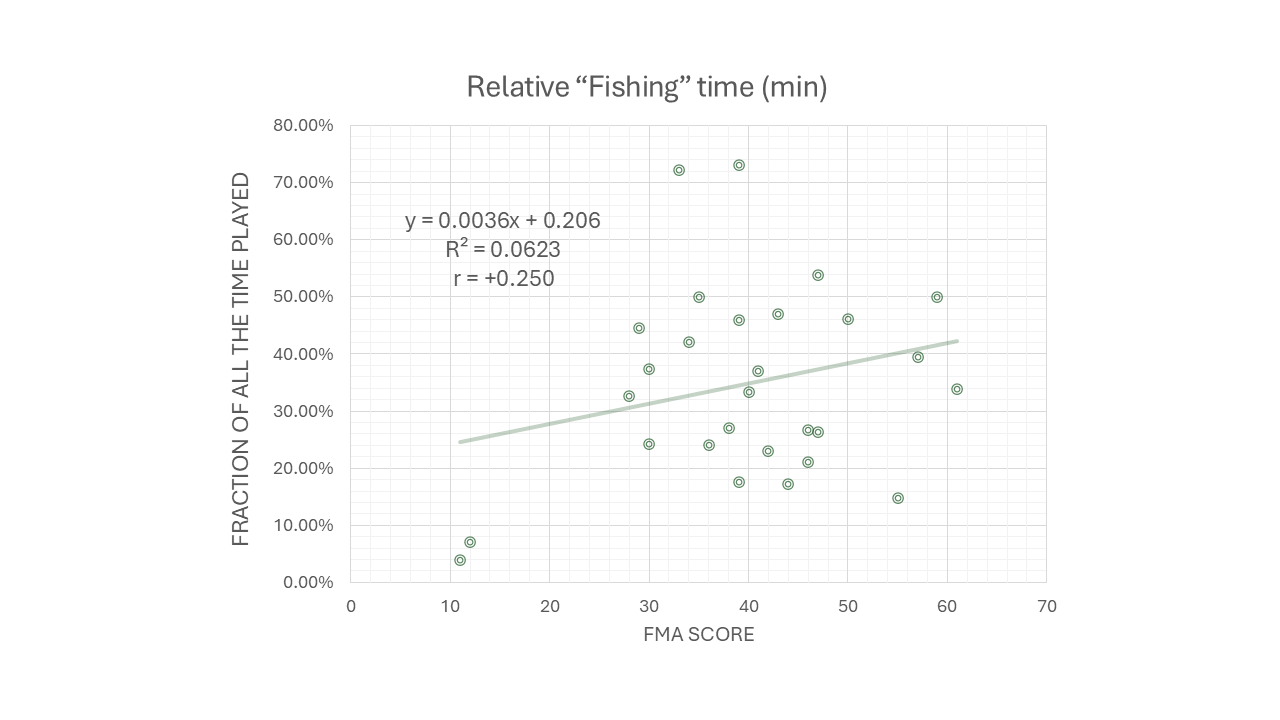
Figure 3. Graphs depicting preference for playing one of three games. a) Rise of the Phoenix; b) Fishing; c) Place the cubes. Each circle represents a chronic stroke survivor. X-axis shows their FMA score - the measure of their impairment: the more the FMA the more mobile they are. Y-axis shows time they played a certain game as a fraction of all the play time. a) and c) have moderate but opposite correlations; whereas b) doesn’t have any significant correlation.
Rehabilitation is not one-size-fits-all. And XR rehabilitation shouldn’t be either.
A lot of review papers exploring how VR affects stroke recovery don’t discriminate between “immersive” or “non-immersive virtual reality”. This in itself poses an analysis problem since immersion in VR brings so much more presence, embodiment and engagement than a flat screen of “non-immersive VR”. What we found, however, is that the same immersive VR, within the same application, can lead to different results because different games are preferred by different patients. And we can design those games with different impairments in mind!
More Impairment = More Stimulation
Another clear trend emerged from the data:
Participants with lower Fugl-Meyer scores generally required:
more stimulation time (Figure 4a),
and higher stimulation intensities (Figure 4b).
Again, clinically intuitive, but now measurable inside a real-time XR environment.
This opens interesting possibilities for:
adaptive therapy systems,
movement analytics,
progress tracking,
and eventually AI-assisted rehabilitation personalization.


Figure 4. a) How long did each participant receive stimulation during the experience, as a fraction of all the time played. b) What was the highest stimulation each participant receive during the experience. All of that - as a function of FMA
We’re Excited
This study was not designed to prove clinical efficacy.
We’re not claiming neuroplastic miracles after one session.
But what we did demonstrate is important:
stroke survivors engaged with the system,
therapists could realistically use it,
different games supported different impairment levels,
and XR + FES can create a responsive, adaptive rehabilitation environment.
Most importantly: participants were willing to stay engaged for meaningful therapy durations.
What Comes Next
We’re now moving toward:
longitudinal studies,
home rehabilitation trials,
biomechanical movement analytics,
adaptive stimulation systems,
and more personalized rehabilitation experiences.
The long-term ambition is to create rehabilitation systems that are:
intensive,
engaging,
adaptive,
and accessible beyond specialist clinics.
If you’re working on:
neurorehabilitation,
movement science,
FES,
XR,
biomechanics,
or home rehabilitation,
we’d genuinely love to talk.
And if you happen to have strong opinions about virtual fish - get in touch.